We will use two public datasets (StrokeFAIR and SOOP) to train and test models to predict functional domains that compose NIHSS in patients with acute ischemic strokes. NIHSS is a key metric for assessing the clinical impact of acute strokes and is critical for treatment decisions and prognostic modeling. The automated calculation of NIHSS supports practical aspects of patient care and serves as a basis for evaluating functional impairment. Predicting functional outcomes by integrating image and non-image features advances our understanding of the brain functions and aids in identifying biomarkers of brain health. Additionally, we will develop cloud-based services to calculate NIHSS domains, which will be user-friendly and provide real-time results. We will also generate a feature set from over 3,500 patients, which will be publicly available for hypothesis testing, reproducibility, and new resource development. The tools will be accessible to promote the democratization of science.
We will analyze two large public datasets of patients with acute ischemic stroke. The training set, StrokeFAIR (Annotated Clinical MRIs and Linked Metadata of Patients with Acute Stroke), includes 2,888 images and metadata, with 1,888 ischemic strokes. This data is public at the Inter University Consortium for Political and Social Research, ICPSR (https://www.icpsr.umich.edu/web/ICPSR/studies/38464) and, together with other resources we developed for automatic analysis of stroke images, won the Dataworks 2023 Exemplary Achievement Award. The testing set, the Stroke Outcome Optimization Project (SOOP), includes 1,700 patients with ischemic strokes, available at Open Science Framework (OSF), a GREI. For both datasets, we will use stroke core annotations, DWI and FLAIR images, demographic data, clinical profiles, and NIHSS scores (total and by domain) collected at admission.
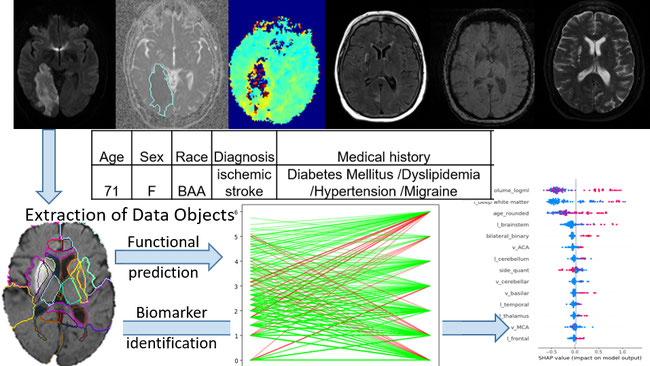
After harmonizing space and intensity to align images and reduce inter-database variance, we will encode the data to decrease dimensionality while preserving biological relevance. The inputs will include several image and non-image domains: 1) quantitative vectors of affected regions generated from 3D annotations of the stroke core, atlases, and technology we have developed; 2) disconnectome maps indicating the probability of injury in brain connections affected by the stroke; 3) multimodal MRIs providing insights into the stroke lesion and the overall status of the brain; and 4) metadata representing demographic and clinical profiles of the populations. With these inputs, we will create a compact feature space that effectively represents multi-modal data.
Most of the training data (~1,500 cases) include NIHSS domain-specific labels. Using the feature space, we will train models to predict NIHSS domains, and test them on the external SOOP dataset. We will likely use a combination of unsupervised machine learning models (e.g., random forest), and supervised neural networks (e.g., deep learning) to train and validate the models. The independent test set will provide insights into model robustness and generalization. Feature analysis, using methods like Mean Decrease Impurity (MDI) and SHAP, will identify important predictors for the general model and explanatory variables for individual scores.
The datasets are well-curated, organized in BIDS format, and ready for analysis, reducing the time typically spent on data preparation. We estimate three months for data curation and harmonization, six months for modeling, training, and testing, and three months for final model refinement, integration into ADS (a user friend free toolbox for stroke analysis), and data and resource sharing in OSF, Vivli, and NITRC. Results will also be published during the final phase
This project follows an Open Science approach, utilizing reusable data from two open-source datasets and producing accessible, reusable resources for a broad user community. The project outputs will include:
1) An accurate model to predict acute functional impairment (NIHSS) after brain stroke, generalizable to external clinical data
2) Identification of relevant image and non-image features that influence the acute impairment, which potentially serve as basis for neuroscientific studies and biomarker search.
3) User-friendly, public software for NIHSS prediction and feature analysis.
4) A feature space of over 3,500 acute ischemic stroke patients, integrating image and non-image data.
5) A web service where users can process their data and calculate predicted NIHSS scores (total and per domain).
All resources, including scripts, feature space matrices, and test results, will be shared publicly via OSF, Vivli, Nitrc and GitHub. This continues our previous open-access work, which includes the release of the first large dataset of patients with acute stroke, the StrokeFAIR dataset (https://www.icpsr.umich.edu/web/ICPSR/studies/38464), the sharing of the first 3D digital atlas of brain arterial territory (https://www.nitrc.org/projects/arterialatlas), and the Acute stroke Detection and Segmentation tool, ADS (https://www.nitrc.org/projects/ads).
Aligned with FAIR principles, the resources that will result from the current project will be findable and accessible in public repositories, interoperable through numerical matrices compatible with various models, APIs, and image analysis tools, and the outputs will be reusable for creating or testing new models.
By releasing both the data and analytical tools in a user-friendly format, we enable not only expert computational scientists but also clinical researchers from diverse fields—who may not be experts in image or computer sciences—to utilize our resources. This allows them to test the replicability and reproducibility of our models, as well as their own prospective work. Researchers can use our feature space as a test set for their hypotheses and apply their data to evaluate the reliability and generalization of our models.
Like our previous tools and resources, our aim is to enhance reproducibility and generalization in research while democratizing science. We provide state-of-the-art tools that empower scientists across various disciplines to effectively analyze image and clinical data, transforming this process from a nuisance into a viable means for investigating their questions. Although reusing clinical data increases technical complexity, it also enhances the potential for generalizing tools and results, allowing for the effective use of the vast clinical data generated daily and increasing the direct impact on clinical care.
The significance of the models, tools, and data produced here is threefold:
First, we will develop a simple, user-friendly system for calculating NIHSS by domain. NIHSS is widely used in hospitals for managing acute ischemic stroke patients, with authorities requiring a baseline score before any intervention and within 12 hours for untreated patients. NIHSS calculation takes about 10 minutes, which is significant in urgent cases. Although inter-evaluator agreement is generally high, a study showed NIHSS scores varied by up to 5 points between emergency and neurology experts, with differences of 3 points or more in 26% of patients and 2 points or more in 54%. An automated system providing real-time NIHSS scores can speed up the process, serve as a second evaluator, and aid in triaging when specialists aren't available. Automated reports could also produce structured text, easing future AI and NLP applications, such as predictive models for recovery (in which NIHSS is one of the most important variables to consider) or flagging patients needing special attention due to unexpected functional responses.
Second, and perhaps most significant from a neuroscience perspective, we will identify features that predict NIHSS. The global NIHSS score, a composite of 11 functional domains, may not pinpoint specific functional impairments due to the spatial localization of brain functions. By using domain-specific NIHSS scores, we can identify features relevant to individual functional domains, providing insights into brain function and intercommunication. Additionally, by including both image and non-image data, we can explore how demographic and clinical factors, like age, pre-existing conditions, or brain atrophy, influence functional outcomes. This is critical for identifying factors contributing to "brain health," a growing but underexplored area.
Third, we will release encoded data as a testbed for researchers and developers. Since StrokeFAIR and SOOP are publicly available without restrictions, and our generated data (lesion loading, connectomes, anonymized lesions) is not classified as human data, it can be openly shared. This biobank will allow researchers across various fields to train and test models, and developers in computational science or biomedical engineering to build new tools. This initiative supports resource democratization, benefiting a broad range of users.
Our team is multidisciplinary. The PI, Dr. Faria, is a trained radiologist with over 20 years of experience in neuroscience and image analysis. A pioneer in cloud-based systems (e.g., MRICloud) and brain atlas development, she focuses on biologically relevant regions of interest. Dr. Faria also created the first large dataset of acute stroke patients and developed user-friendly, privacy-conscious tools for automatic lesion segmentation. As a Latin woman and first-generation college graduate, she is a strong advocate for diversity in research, promoting inclusivity within both research subjects and teams. She is also a leader in open science, reproducibility, and generalization.
This project combines medical, bioengineering, and data science expertise. Dr. Liu and Dr. Abdeltawab are experts in software and biomedical engineering, leading model and tool development. Ms. Zhang, a skilled student in computational analysis, adds valuable support. Together, this team is well-positioned to advance the research and expand open science for researchers and participants alike.
The key to this project's success is access to a large, well-curated, and well-documented sample of patients, including multimodal data (neuroimaging, demographic, and clinical information) for model training and hypothesis testing. Equally important is the expertise of researchers from diverse fields (which our team has) and experience in conducting experiments, releasing data, and sharing resources following FAIR principles. Tackling a clinically relevant issue, such as acute stroke—the leading cause of disability worldwide—further strengthens the project's impact. Thus, this proposal succeeds by addressing the core factors for problem-solving: relevance, available technology, and implementation viability.
